Alleviation: An International Journal of Nutrition, Gender & Social Development, ISSN 2348-9340 , Volume 8, Number 8 (2021): 1-5
© Arya PG College (College with Potential for Excellence Status by UGC) & Business Press India Publication, Delhi
http://apcjournals.com, www.aryapgcollege.ac.in
Effectiveness of Nutraceuticals in the Management and Prevention of Rheumatoid Arthritis
Mamta Sharma
Assistant Professor, Department of Home Science
Geeta Degree College, Shera
Panipat (Haryana), India
Email: r.kaushik82@gmail.com
Abstract
Rheumatoid arthritis (RA) is a chronic inflammatory condition marked by high levels of oxidative stress and inflammatory biomarkers. Because of the severe adverse effects of the drugs used to treat the disease, new and safe treatments are needed. Food contains phenolic compounds, polyunsaturated fatty acids, phytosterols, tocopherols, and carotenoids, all of which are antioxidants and have anti-inflammatory bioactive ingredients. Because of the risks connected with synthetic medications, the usage of nutraceuticals and supplements is on the rise. Clinicians are aware of these treatments and may prescribe nutraceuticals in addition to the standard of care. The effects of nutraceuticals in rheumatoid arthritis have been proven in several scientific research, meta-analyses, and randomised clinical trials. The majority of nutraceuticals that have a favourable effect on chronic inflammatory disorders are discussed in this review, along with evidence for their efficacy and mechanism of action.
Keywords: Biomarkers, Fish Oil, Glucosamine, Inflammation, Nutraceuticals, Rheumatoid Arthritis
Introduction
Rheumatoid Arthritis (RA) is the most common autoimmune illness, characterized by an autoimmune response that leads to synovial joint damage. Progressive disability, systemic problems, and untimely death are all linked to RA. Uncontrolled active RA, in particular, causes joint deterioration, disability, a lower quality of life, as well as cardiovascular and other co-morbidities. Rheumatoid arthritis affects about 1 per cent of adults worldwide, with women being 2-3 times more likely than males to develop the disease. RA is more common as one gets older, until one is around 70 years old. In developing countries, the risk of having RA peaks is at a younger age, while the exact age varies by location.
The goal of pharmacological treatment for RA is to stop the disease from progressing further by alleviating symptoms with disease-modifying anti-rheumatic medications.
Alternative therapies, such as nutraceuticals and vitamins, are becoming more popular in the treatment of rheumatoid arthritis. Nutraceuticals are foods or products that have the potential to improve one's health and provide relief from certain medical conditions. Nutraceuticals are defined by the European Nutraceutical Association as "nutritional products with health-related effects." These are not manmade substances or chemical compounds produced for specific indications, unlike medications. These are "food products" that contain nutrients partially in concentrated form. Glucosamine, chondroitin, krill oil, fish oil, gamma linolenic acid, and avocado-soybean unsaponifiables are some of the most extensively used nutraceuticals in joint diseases (McInnes & Schett 2011, Vista & Lau 2011).
Several clinical trials have been conducted to determine the efficacy of these products, but the findings have been mixed. Because of their popularity, clinicians should be aware of these nutraceuticals and have a basic understanding of these.
Pathogenesis of Rheumatoid Arthritis
Synovial inflammation and hyperplasia, autoantibody production, cartilage and bone loss are all symptoms of rheumatoid arthritis. The molecular aetiology of RA shows a complicated interplay between hereditary and environmental variables that leads to a convoluted autoimmune response when the underlying event activates the disease. More than 30 loci associated in RA pathogenesis have been found in large genome-wide association studies. HLA (e.g. DRB1*01, DRB1*04, DRB1*13, and DRB1*15) and non-HLA (e.g. PTPN22, IL23R, TRAF1, CTLA4, IRF5, STAT4, CCR6, PADI4) genes are known to predispose to RA heredity, with HLA genes contributing more to RA heritability, while environmental factors have also been linked to RA susceptibility (Figure 1).
The onset of an autoimmune response is critical to comprehending RA since it is the result of a complex gene-environment interaction that leads to the loss of immunological tolerance and subsequent synovial micro environmental alterations. Through complicated cell-cell interactions (including local dendritic cells that express cytokines, HLA class II molecules, and co-stimulatory molecules), an imbalanced immune system provides the molecular stimulation required for T-cell activation and proliferation. Antigen presentation and 'T-cell-mediated B-cell assistance' come from T-cell activation, which activates B cells and macrophages. Macrophages are synovitis' main effectors, releasing cytokines (e.g., TNF- and interleukin-1, 6, 12, 15, 18, 23), producing prostanoids and matrix-degrading enzymes, phagocytosis, and antigen presentation. Pro-inflammatory cytokines such as interleukin-1 and tumour necrosis factor (TNF) drive articular cartilage synovial fibroblasts and chondrocytes to release enzymes that breakdown proteoglycans and collagen, resulting in tissue degradation (Arend 1997). Apart from cytokines, reactive oxygen and nitrogen intermediates cause oxidative stress, which is implicated in the breakdown of cartilage, extracellular collagen, and intracellular DNA, while antioxidants and oxidative enzymes have been proved to alleviate arthritis (Hitchon & El-Gabalawy 2004).
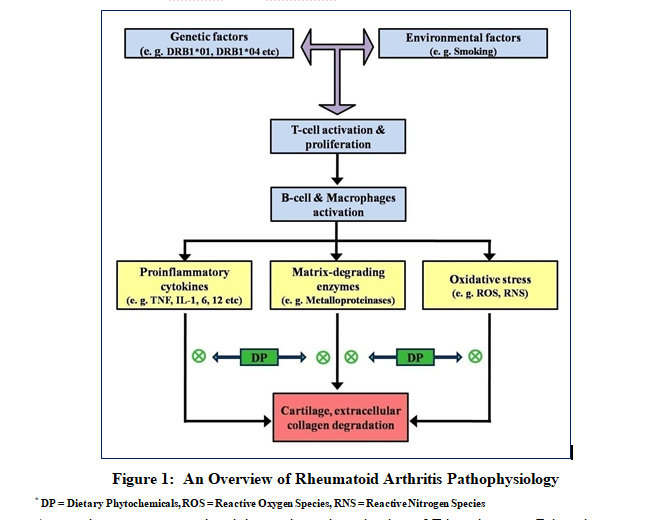
An autoimmune response involving pathogenic activation of T-lymphocytes, B-lymphocytes, and macrophages is predisposed by an intricate interaction between a variety of hereditary and environmental variables. Such pathogenic immune activation results in oxidative stress, inflammation, and activation of matrix degrading enzymes, all of which contribute to RA symptoms such as cartilage degeneration, extracellular collagen breakdown, and so on.
Various Nutraceuticals in the Management of Rheumatoid Arthritis
1) Glucosamine
Glucosamine is an amino-saccharide found in the human body. It's required for the manufacture of proteoglycan, which is crucial for cartilage integrity. Matrix metalloproteinases, Interleukin-1, COX-2, and proteoglycan are all inhibited by it. At a recommended amount of 1500 mg per day, it is one of the most often taken supplements in patients. Many formulations contain glucosamine, however the sulphated version is more widely utilized in clinical trials. A lot of research has been done on glucosamine and chondroitin, or a combination of the two. Minimal side effects and probable therapeutic improvement of symptoms are two potential benefits of glucosamine use. Glucosamine is thought to be safe because no major or fatal side effects have been reported (Henrotin et al 2012).
In patients with asthma or shellfish allergies, however, it should be taken with caution (Chou et al 2005). Various randomised control trials indicate contradictions in the results, raising issues about its efficacy in joint arthritis in the literature. In patients with knee or hip osteoarthritis (OA), a recent meta-analysis of 3,803 patients compared glucosamine, chondroitin, and placebo in patients with OA (Wandel 2010). These smaller trials found that glucosamine, chondroitin, and their combination do not decrease joint discomfort or slow disease development when compared to placebo. Other research, on the other hand, have suggested that combining glucosamine and chondroitin had a synergistic benefit in a minority of patients. The glucosamine/chondroitin Arthritis Intervention Trial enrolled 1,583 patients in a multicenter, participant and investigator masked study. Participants had to be at least 40 years old and have clinical and radiographic evidence of OA to be considered. The patients were subsequently randomly randomised to receive glucosamine, chondroitin, a combination of the two, or a placebo (Clegg et al 2006). Overall, there was no discernible improvement in pain reduction. However, when glucosamine and chondroitin were combined, pain was reduced in the subgroup with moderate to severe illness. Glucosamine did not relieve pain when compared to placebo in a Cochrane analysis of 4926 patients in 25 randomized control trials (Towheed 2006). The routes and quantities utilized varied widely, and only the commercially financed studies demonstrated improvement with glucosamine; nonetheless, inadequate allocation concealment must be acknowledged.
2) Chondroitin
The primary component of aggrecan, which is part of the cartilage ultrastructure is chondroitin (Chou et al 2005). The majority of the preparations are made from cartilaginous animal extracts (Ronca et al 1998). It is most typically marketed as chondroitin sulphate, a nutraceutical-grade substance made up of alternating N-acetyl-D-galactosamine and D-glucuronic acid chains similar to glucosamine (Reginster et al 2005). Although some studies claim that it inhibits matrix metalloproteinases, Interleukin-1 (IL-1), increases cyclooxygenase (COX)-2, and stimulates proteoglycan synthesis, the specific mechanism of action is unknown. Anti-inflammatory, anticatabolic, antiapoptotic, and antioxidant properties have been demonstrated in vitro animal experiments. However, human models have yet to be directly extrapolated (Chan et al 2005, Olsen et al 2010, Ronca et al 1998). Again, there are inconsistencies in the literature addressing the clinical value of chondroitin. A meta-analysis of 20 trials found that chondroitin sulphate was effective for hip and knee osteoarthritis in 3846 patients (Reichenbach et al 2007). Although conclusive assessment was difficult due to a large degree of heterogeneity as well as the small and low quality of the trials, the authors concluded that chondroitin showed minor or no symptomatic benefits and advised against its usage. At an 800 mg daily dose, chondroitin reduced the rate of reduction in joint space width, according to a recent meta-analysis of three RCTs (Hochberg 2010). In the short term, chondroitin (alone or in combination with glucosamine) was found to be better than placebo in individuals with osteoarthritis in a Cochrane systematic review of 9,110 patients from 43 studies of randomised trials (Singh et al 2015). The majority of the research focused on knee osteoarthritis, with follow-up periods ranging from one month to three years. In 11 of the studies with a duration of less than 6 months, chondroitin alone or in combination with glucosamine was found to be substantially more effective in improving pain levels than the comparator. When comparing chondroitin to placebo, however, studies with lower sample sizes of less than 100 individuals showed no statistically significant reduction in pain levels when stratified by study size. Only three of the 11 studies had sample sizes of more than 100 people. When trials were classified further, those that were commercially financed scored much higher on pain than those that were not. Based on data of moderate to high quality, there was significantly lower decline in minimal joint space width with chondroitin compared to placebo groups. There were no adverse effects reported, implying that chondroitin is well tolerated. Despite this, the most recent American Academy of Orthopaedic Surgeons
(AAOS) advises against using chondroitin in therapeutic settings.
3) Vitamin E
Vitamin E (Fat-Soluble Vitamin) helps to maintain bone integrity, energy production, and anti-oxidant activity while also increasing immunity against many diseases (Riccioni et al 2003). By scavenging free radicals, dietary anti-oxidants limit oxidative damage, which is the most common cause of inflammatory disease. It possesses anti-oxidant properties, and because of its protective role, decreasing serum concentrations may increase vulnerability to rheumatoid arthritis. Many scientific trials have shown that Vitamin E can help with rheumatoid arthritis. With vitamin E, there were no negative side effects.
4) Omega-3 Fatty Acids
Fish oil, flaxseed, and other dietary supplements provide omega-3 fatty acids - Omega 3 fatty acids exist in α-linolenic acid, eicosapentaenoic acid, and docosahexaenoic acid Plant oils, such as flaxseed, soybean, and canola oils, are high in α-linolenic acid, whereas fish and other shellfish have docosahexaenoic acid and eicosapentaenoic acid (Kris-Etherton 2002). The synthesis of pro-inflammatory cytokines, cartilage degrading enzymes, and arachidonic acid is reduced when omega-3 fatty acids are increased. The tumour necrosis factor is reduced when arachidonic acid is reduced. Many studies have found that combining omega-3 supplements with regular rheumatoid arthritis treatment, rather than medicine alone, can help control rheumatoid arthritis. It was also observed that using omega 3 supplements along with anti-rheumatic medicine can help those with newly diagnosed rheumatoid arthritis have fewer symptoms and require less pain medication.
5) Krill Oil
Antarctic krill (Ephausia Superba), a kind of zooplankton rich in phospholipids, is used to make krill oil. It has a high concentration of n-3 fatty acids, similar to fish oil. However, only a few researches have looked into the effects of krill oil. In comparison to control mice, arthritis-induced animals fed a krill oil supplemented diet had considerably lower arthritis scores, inflammatory cell infiltration into the joint, and hind paw swelling. The administration of krill oil appears to be beneficial in a randomised, double-blind, controlled study of 90 patients (Deutsch 2007). Patients with verified cardiovascular disease, RA, and OA, as well as elevated C-reactive protein levels (CRP), were chosen. CRP levels, discomfort, and functional impairment scores were all significantly lower in patients who took krill oil. There were no reported side effects in patients who used krill oil. Despite its growing popularity, more research into the possible advantages in human studies is required.
6) Fish Oil
Omega-3 polyunsaturated fatty acids are found in fish oil. It's made from the flesh of fatty fish and includes essential fatty acids for biological activities. It's suggested to affect metabolic pathways by lowering the overall inflammatory response (Caughey et al 2010). It can also be used as a long-term adjunct or a way to lessen the use of other analgesics (Fortin 1995). Patients are frequently advised to stop taking fish oil weeks before surgery. The evidence for this is shaky, and more research is needed. Although fish oil may have a minor antiplatelet impact, a recent meta-analysis found no evidence of an increased risk of significant bleeding after surgery (Xin et al 2013).
7) Gamma Linolenic Acid (GLA)
Gamma linolenic acid is a kind of omega-6 fatty acid. Gamma linolenic acid is an important fatty acid that can be found in blackcurrant, primrose, and borage seed oils (Zurier 1996). A recent cochrane review examined seven trials on the effects of GLA in RA (Cameron 2011). Small (525-540 mg) and large (1.4-2.8 g) dosage groups and time periods were used in the experiments. The most benefit appeared to be from dosages of 1.4 g/day for at least 6 months, which improved self-reported Visual Analogue Scale (VAS) pain scores statistically significantly. Unlike the other authors, who claimed that primrose oil causes hypersensitive reactions or seizures in patients.
8) Avocado-Soybean Unsaponifiables (ASUs)
Unsaponifiable fractions of one-third avocado oil and two-thirds soybean oil are used to make ASUs ( Maheu et al 2014). These exhibit anabolic, anti-catabolic, and anti-inflammatory actions on chondrocytes, as well as inhibiting spontaneous and IL-1-induced collagenase activity, all of which are regarded to be beneficial in osteoarthritis patients (Ernst 2003). The impact of ASUs on knee and hip osteoarthritis was studied in four Randomized Controlled Trials (RCTs) and one systematic review. The data for ASUs were the most comforting of the herbal medicines studied. After three months of follow-up, ASUs reduced non-steroidal anti-inflammatory drugs intake in three trials. In another investigation, ASUs and chondroitin sulphate were compared in knee osteoarthritis. After a 6-month follow-up period, it was discovered that there was no difference between the two groups, with 361 patients enrolled. Maheu et al (2014) enrolled 399 individuals with symptomatic hip OA in their study. The ASU and placebo groups had no statistically significant differences in mean joint space width; however, the ASU group had a 20 per cent lower rate of progression, which was not statistically significant. This shows that ASUs may have the ability to delay the course of osteoarthritis.
9) Chicory
Cichorium intybus (Chicory) is a perennial herb that has been utilised for numerous therapies in nations such as India, Afghanistan, Bosnia and Herzegovina, Bulgaria, Iran, Italy, Jordan, Morocco, Pakistan, Poland, Serbia, South Africa, and Turkey (Street et al 2013). It reduces inflammation by inhibiting the formation of prostaglandin E2 (PGE2) and increasing the activation of B cells (NF-kB) expression (Al-Snafi 2016). It also has antioxidative and glucosidase inhibitory effects (Abd El-Wahab et al 2013, Carazzone et al 2013). At a dose of 600 mg to 1800 mg per day for one month, a placebo-controlled, double-blind chicory root extract experiment indicated relief in pain and stiffness among hip or knee osteoarthritis patients (Olsen et al 2010). Chicory should not be consumed during pregnancy or nursing
(Ema 2010).
10) Devil’s Claw
Harpagophytum procumbens (Devil's Claw) contains iridoid glycoside, which possesses anti-inflammatory, anti-rheumatic, and analgesic activities (Park 2016). The iridoid glycoside suppresses the release of TNF, COX-2, Interleukin-6, Interleukin-1, and prostaglandin E2 (Fiebich et al 2012) and limits the production of inflammatory cytokines (Liu and Wang 2011). With a daily dose of 2610 mg, it was found to be a well-tolerated and effective treatment for mild to severe rheumatic illnesses (degenerative) in a research (Leblan et al 2000). Another study comparing Harpagophytum procumbens to 100 mg diacerein found no significant differences (Cuspidi 2015 & Kris-Etherton et al 2002). Despite the fact that numerous clinical research have inferred devil’s claw usefulness in pain therapy, many studies still require more adequate confirmatory studies for the treatment guidelines (Chrubasik et al 2004).
Conclusion
The use of nutraceuticals in the treatment of rheumatoid arthritis (RA) is becoming more popular. This is a quick rundown of some of the most popular goods. Overall, there isn't much evidence that using these products can slow down the progression of RA. Some of these drugs, on the other hand, appear to relieve pain and enhance function in some people. The undesirable effects and potential advantages of these products must be considered before prescribing or counselling regarding their usage. More research is needed to standardise results and give larger data sets with more controlled processes. Patients and physicians must be able to make well-informed decisions regarding the use of these nutraceuticals based on scientific, medical, and financial data.
References
Abd El-Wahab AE, Ghareeb DA, Sarhan EE, Abu-Serie MM and Demellawy MA (2013) In Vitro Biological Assessment of Berberis Vulgaris and Its Active Constituent, Berberine: Antioxidants, Antiacetylcholinesterase, Anti-Diabetic and Anticancer Effects. BMC Complementary and Alternative Medicine 13 (1) : 218.
Al-Snafi AE (2016) Medical Importance of Cichorium Intybus–A Review. IOSR Journal of Pharmacy 6 (3) : 41 - 56.
Arend W (1997) The Pathophysiology and Treatment of Rheumatoid Arthritis. Arthritis Rheum 40 (4) : 595 - 597.
Cameron M, Gagnier JJ and Chrubasik S (2011) Herbal Therapy for Treating Rheumatoid Arthritis. Cochrane Database Syst Rev: CD002948.
Cantaert T, Brouard S and Thurlings RM (2009) Alterations of the Synovial T Cell Repertoire in Anti-Citrullinated Protein Antibodypositive Rheumatoid Arthritis Arthritis Rheum 60 : 1944 - 1956.
Carazzone C, Mascherpa D, Gazzani G and Papetti A (2013) Identification of Phenolic Constituents in Red Chicory Salads (Cichorium Intybus) by High-Performance Liquid Chromatography with Diode Array Detection and Electrospray Ionisation Tandem Mass Spectrometry. Food Chemistry 138 (2 - 3) : 1062 - 1071.
Caughey GE, James MJ, Proudman SM and Cleland LG (2010) Fish Oil Supplementation Increases the Cyclooxygenase Inhibitory Activity of Paracetamol in Rheumatoid Arthritis Patients. Complement Ther Med 18 : 171 - 174.
Chan PS, Caron JP and Orth MW (2005) Effect of Glucosamine and Chondroitin Sulfate on Regulation of Gene Expression of Proteolytic Enzymes and their Inhibitors in Interleukin-1-Challenged Bovine Articular Cartilage Explants. Am J Vet Res 66 : 1870 - 1876.
Chou MM, Vergnolle N, McDougall JJ, Wallace JL and Marty S (2005) Effects of Chondroitin and Glucosamine Sulfate in a Dietary Bar Formulation on Inflammation, Interleukin-1beta, Matrix Metalloprotease-9, and Cartilage Damage in Arthritis. Exp Biol Med (Maywood) 230 : 255 - 262.
Chrubasik S, Conradt C and Roufogalis BD (2004) Effectiveness of Harpagophytum Extracts and Clinical Efficacy. Phytotherapy Research: An International Journal Devoted to Pharmacological and Toxicological Evaluation of Natural Product Derivatives 18 (2) : 187 - 189.
Clegg Do, Reda DJ, Harris CL, Klein MA and O’Dell JR (2006) Glucosamine, Chontroitin Sulphate and the Two Combination for Painful Knee Osteoarthritis. N Engl J Med 354 : 795 - 808.
Clements JN (2011) Treatment of Rheumatoid Arthritis: A Review of Recommendations and Emerging Therapy. Formulary 46 (12).
Costenbader K, Chang S, Laden F, Puett R and Karlson EW (2008) Geographic Variation in Rheumatoid Arthritis Incidence among Women in the United States. Arch Intern Med 168 : 1664 - 1670.
Cuspidi C, Sala C, Tadic M, Grassi G and Mancia G (2015) Systemic Hypertension Induced by Harpagophytum Procumbens (Devil's Claw): A Case Report. Journal of Clinical Hypertension (Greenwich, Conn.) 17 (11) : 908 - 910.
Cutolo M, Kitas GD and Riel PL (2014) Burden of Disease in Treated Rheumatoid Arthritis Patients: Going Beyond the Joint. Semin Arthritis Rheum 43 (4) : 479 - 488.
Deutsch L (2007) Evaluation of the Effect of Neptune Krill Oil on Chronic Inflammation and Arthritic Symptoms. J Am Coll Nutr 26 : 39 - 48.
Donahue K, Gartlehner G and Jonas D (2008) Systematic Review: Comparative Effectiveness and Harms of Disease-Modifying Medications for Rheumatoid Arthritis Ann Intern Med 148 : 124 - 134.
Ema H (2010) Community Herbal Monograph on Rosmarinus Officinalis L. Folium. Europe: Committee on Herbal Medicinal Products.
Ernst E (2003) Avocado-Soybean Unsaponifiables (ASU) for Osteoarthritis - A Systematic Review. Clin Rheumatol 22 : 285 - 288.
Fenton JI, Chlebek- Brown KA, Caron JP and Orth MW (2002) Effect of Glucosamine on Interleukin Conditioned Aarticular Cartilage. Equine Veterinary Journal 34 (34) : 219 - 223.
Fiebich BL, Muñoz E, Rose T, Wei G and McGregor GP (2012) Molecular Targets of the Anti Inflammatory Harpagophytum Procumbens (Devil's Claw): Inhibition of TNFα and COX-2 Gene Expression by Preventing Activation of AP-1. Phytotherapy Research 26 (6) : 806 - 811.
Fortin PR, Lew RA, Liang MH, Wright EA and Beckett LA (1995) Validation of a Meta - Analysis: The Effects of Fish Oil in Rheumatoid Arthritis. J Clin Epidemiol 48 : 1379 - 1390.
Goldberg RJ and Katz J (2007) A Meta - Analysis of the Analgestic Effect of Omega Three Polyunsaturated Fatty Acid Supplementation for Inflammatory Joint Pain. Pain 129 : 210 - 223.
Henrotin Y, Mobasheri A and Marty M (2012) Is There Any Scientific Evidence for the Use of Glucosamine in the Management of Osteoarthritis? Arthritis Res Ther 14 (1) : 201.
Hitchon CA and El-Gabalawy HS (2004) Oxidation in Rheumatoid Arthritis. Arthritis Res Ther 6 : 265 - 278.
Hochberg MC (2010) Structure-Modifying Effects of Chondroitin Sulfate in Knee Osteoarthritis: An Updated Meta-Analysis of Randomized Placebo Controlled Trials of 2-Year Duration. Osteoarthritis Cartilage 18 Suppl 1 : S 28 - 31.
James M, Proudman S and Cleland L (2010) Fish Oil and Rheumatoid Arthritis: Past, Present and Future. Proceedings of The Nutrition Society 69 (3): 316 - 323.
Jevesevar DS (2013) Treatment of Osteoarthritis of the Knee: Evidence Based Guidelines J Am Acad Orthop Surg 21 : 571 - 576.
Karlson EW, Shadick NA, Cook NR, Buring JE and Lee IM (2008) Vitamin E in the Primary Prevention of Rheumatoid Arthritis: The Women's Health Study. Arthritis Care & Research 59 (11) : 1589 - 1595.
Kondamudi N, Turner MW and McDougal OM (2016) Harpagoside Content in Devil's Claw Extracts. Natural Product Communications 11 (9) : 1215 - 1216.
Krs-Etherton PM, Harris WS and Appel LJ (2002) Fish Consumption, Fish Oil, Omega-3 Fatty Acids, and Cardiovascular Disease Circulation 106 (21) : 2747 - 2757.
Kurkó J, Besenyei T, Laki J, Glant TT, Mikecz K and Szekanecz Z (2013) Genetics of Rheumatoid Arthritis - a Comprehensive Review. Clin Rev Allergy Immunol 45 (2) : 170-179.
Leblan D, Chantre P and Fournie B (2000) Harpagophytum Procumbens in the Treatment of Knee and Hip Osteoarthritis. Four-Months Results of a Prospective, Multicenter, Double Blind Trial Versus Diacerhein. Joint Bone Spine 67 (5) : 462- 467.
Lebre MC, Jongbloed SL, Tas SW, Smeets TJ, McInnes IB and Tak PP (2008) Rheumatoid Arthritis Synovium Contains Two Subsets of CD 83- DC-LAMP- Dendritic Cells with Distinct Cytokine Profiles. Am J Pathol 172 : 940 - 950.
Lerna M, Kerr A, Scales H, Berge K and Griinari M (2010) Supplementation of Diet with Krill Oil Protects against Experimental Rheumatoid Arthritis. BMC Musculoskelet Disorders 11 : 136.
Little CV and Parsons T (2001) Herbal Therapy for Treating Osteoarthritis. Cochrane Database Syst Rev 1 : CD002947.
Liu X and Wang JM (2011) Iridoid Glycosides Fraction of Folium Syringae Leaves Modulates NF-κB Signal Pathway and Intestinal Epithelial Cells Apoptosis in Experimental Colitis. PLoS One 6 (9) : e 24740.
Loeser RF, Goldring SR, Scanzello CR and Goldring MB (2012) Osteoarthritis: A Disease of the Joint as an Organ. Arthritis and Rheumatism 64 (6) : 1697.
Maheu E, Cadet C, Marty M, Moyse D and Kerloch I (2014) Randomised, Controlled Trial of Avocado-Soybean Unsaponifiable (Piascledine) Effect on Structure Modification in Hip Osteoarthritis: The ERADIAS Study. Ann Rheum Dis 73 : 376 -384.
McAlindon TE, Bannuru RR, Sullivan MC, Arden NK and Berenbaum F (2014) OARSI Guidelines for the Non-Surgical Management of Knee Osteoarthritis. Osteoarthritis Cartilage 22 : 363 - 388.
McInnes IB and Schett G (2011) The Pathogenesis of Rheumatoid Arthritis. J Med 365 : 2205 -2219.
Miller KL and Clegg DO (2011) Glucosamine and Chondroitin Sulfate. Rheum Dis Clin North Am 37 : 103 - 118.
O’Dell JR (2011) Rheumatoid Arthritis. In: Goldman L and Schafer AI (Eds) Goldman's Cecil Medicine. Philadelphia PA: Saunders Elsevier.
Olsen NJ, Branch VK, Jonnala G, Seskar M and Cooper M (2010) Phase 1, Placebo Controlled, Dose Escalation Trial of Chicory Root Extract in Patients with Osteoarthritis of the Hip or Knee. BMC Musculoskeletal Disorders 11 (1) : 156.
Orth MW, Peters TL and Hawkins JN (2002) Inhibition of Articular Cartilage Degradation by Glucosamine-HCl and Chondroitin Sulphate. Equine Vet J Supp 1: 224 - 229.
Park KS (2016) A Systematic Review on Antiinflammatory Activity of Harpagoside. Journal of Biochemistry and Molecular Biology Research 2 (3) : 166 - 169.
Park Y, Lee A, Shim SC, Lee JH, Choe JY, Ahn H and Bae SC (2013) Effect of n-3 Polyunsaturated Fatty Acid Supplementation in Patients with Rheumatoid Arthritis: A 16-Week Randomized, Double-Blind, Placebo-Controlled, Parallel-Design Multicenter Study in Korea The Journal of Nutritional Biochemistry 24 (7) : 1367 - 1372.
Pavelka K, Coste P, Géher P and Krejci G (2010) Efficacy and Safety of Piascledine 300 Versus Chondroitin Sulfate In A 6 Months Treatment Plus 2 Months Observation In Patients with osteoarthritis of the Knee. Clin Rheumatol 29 : 659 - 670.
Rajaei E, Mowla K, Ghorbani A, Bahadoram S, Bahadoram M and Dargahi-Malamir M (2016) The Effect of Omega-3 Fatty Acids in Patients with Active Rheumatoid Arthritis Receiving DMARDs Therapy : Double-Blind Randomized Controlled Trial. Global Journal of Health Science 8 (7) : 18.
Ramos M, Tak P and Lebre M (2014) Fms-like Tyrosine Kinase 3 Ligand Dependent Dendritic Cells in Autoimmune Inflammation. Autoimmun Rev 13 (2) : 117 - 124.
Reichenbach S1, Sterchi R, Scherer M, Trelle S and Bürgi E (2007) Meta-Analysis: Chondroitin for Osteoarthritis of the Knee or Hip. Ann Intern Med 146 : 580 - 590.
Reginster JY, Bruyere O, Fraikin G and Henrotin Y (2005) Current Concept in the Therapeutic Management of Osteoarthritis with Glucosamine. Bull Hosp Jt Dis 63 : 31 - 36.
Riccioni G, D'Orazio N, Menna V and De Lorenzo A (2003) Fat Soluble Vitamins and Immune System: An Overview. European Journal of Inflammation 1 (2) : 59 - 64.
Richmond J, Hunter D, Irrgang J, Jones MH and Levy B (2009) Treatment of Osteoarthritis of the Knee (Nonarthroplastry) J Am Acad Orthop Surg 17 : 591 - 600.
Richy F, Bruyere O, Ethgen O, Cucherat M and Henrotin Y (2003) Structural and Symptomatic Efficacy of Glucosamine and Chondroitin in Knee Osteoarthritis: A Comprehensive Meta-Analysis. Arch Intern Med 163 : 1514 - 1522.
Ronca F, Palmieri L, Panicucci P and Ronca G (1998)Anti-Inflammatory Activity of Chondroitin Sulfate. Osteoarthritis Cartilage 6 Suppl A : 14 - 21.
Schroder AE, Greiner A, Seyfert C and Berek C (1996) Differentiation of B Cells in the Nonlymphoid Tissue of the Synovial Membrane of Patients with Rheumatoid Arthritis. Proc Natl Acad Sci USA 93 : 221-225.
Scott DL, Frederick WF and Huizinga TWJ (2010) Rheumatoid Arthritis Lancet 376 (97460) : 1094 - 1108.
Singh JA, Noorbaloochi S, MacDonald R and Maxwell LJ (2015) Chondroitin for Osteoarthritis. Cochrane Database Syst Rev 1 : CD005614.
Street RA, Sidana J and Prinsloo G (2013) Cichorium Intybus: Traditional Uses, Phytochemistry, Pharmacology and Toxicology. Evidence-Based Complementary and Alternative Medicine Doi : 10.1155/2013/579319.
Symmons D, Mathers C and Pfleger B (2006) The Global Burden of Rheumatoid Arthritis in the Year 2000. Geneva : WHO.
Tou JC, Jaczynski J and Chen YC (2007) Krill for Human Consumption: Nutritional Value and Potential Health Benefits. Nutr Rev 65: 63 - 77.
Towheed T, Maxwell L, Anastassiades TP, Houpt J and Welch V (2006) Glucosamine Therapy for Treating Osteoarthritis. Cochrane Database of Syst Rev 2 : CD002946.
Unger M and Frank A (2004) Simultaneous Determination of the Inhibitory Potency of Herbal Extracts on the Activity of Six Major Cytochrome P450 Enzymes Using Liquid Chromatography/Mass Spectrometry and Automated Online Extraction. International Journal of Pharmaceutical Research 18 (19) : 2273 - 2281.
Vista Es and Lau CS (2011) What about supplementation for osteoarthritis? A critical and evidenced –based review Int J Rheum Dis 14 : 152-158.
Wandel S, Juni P, Tendal B, Nuesch E and Villiger PM (2010) Effect of Glucosamine, Chondroitin or Placebo in Patient with Osteoarthritis of Hip or Knee: Network Meta-Analysis BMJ 341 : 4675.
Warnock M, McBean D, Suter A, Tan J, and Whittaker P (2007) Effectiveness and Safety of Devil's Claw Tablets in Patients with General Rheumatic Disorders. Phytotherapy Research : An International Journal Devoted to Pharmacological and Toxicological Evaluation of Natural Product Derivatives 21 (12): 1228 - 1233.
Xin W, Wei W, Lin Z, Zhang X and Yang H (2013) Fish Oil and Atrial Fibrillation after Cardiac Surgery: A Meta-Analysis of Randomized Controlled Trials. PLoS One 8 : e72913.
Zurier RB, Rossetti RG, Jacobson EW, DeMarco DM and Liu NY (1996) Gamma-Linolenic Acid Treatment of Rheumatoid Arthritis. ARandomized, Placebo-Controlled Trial. Arthritis Rheum 39 : 1808 - 1817.